I specialise in cornea surgery and did the first no-suture cornea transplant in the UK in 2003. This article explains how I perform modern cornea transplantation and how partial cornea transplants have greatly improved outcomes for diseases such as Fuchs and keratoconus.
Daily Mail on Fuchs
About the cornea
The cornea is the transparent ‘front window’ of the eye and is also an important focusing structure: any change in its shape or transparency will reduce vision.
What is cornea transplantation?
Some diseases damage the cornea so badly that the only treatment is to replace it with a new, normal cornea. Examples are keratoconus and Fuchs. Cornea transplantation is the replacement of the patients’ own cornea with one donated by a deceased person. It is the same in principal as a kidney or heart transplant although cornea transplantation is a ‘smaller’ operation because it is much less stressful for the body and it is not necessary to take tablets to prevent the new cornea rejecting.
The donor corneas are supplied by United Kingdom Transplant located in Bristol, England or equivalent centres in the USA and are of the highest quality. For example, corneas from donors with transmissable diseases are excluded.
You may come across the term ‘keratoplasty’ which means the same as cornea transplantation.
Different types of cornea transplantation
There are several types of cornea transplantation. They generally involve the removal of a circular area from the centre of the patient’s own cornea and its replacement by the transplant. Cataract surgery may be done at the same time if necessary. Like all operations, cornea transplantation entails some risk and should only be done when absolutely necessary.
Partial cornea transplantation for keratoconus (‘deep anterior lamellar keratoplasty’)
This method saves some of the patient’s own cornea and only replaces the outer layer. This is ideal in keratoconus because in many cases it is only the outer layer of the cornea (called the ‘stroma’) that is abnormal whilst the inner layer (called the ‘endothelium’) is healthy. Preserving the patient’s healthy endothelium is important as it greatly reduces the risk of transplant rejection.
I always perform partial or ‘deep anterior lamellar keratoplasty’ when it is possible to do so. However if the keratoconus is too advanced, for example the cornea is severely scarred, this surgery may not be possible and full thickness or ‘penetrating keratoplasty’ is done instead.
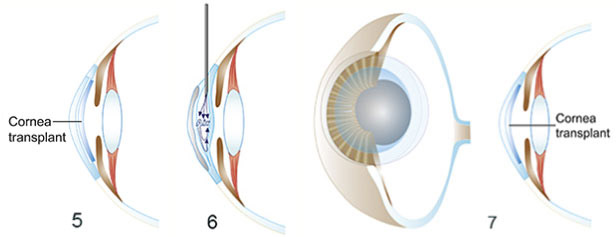
These illustrations of partial cornea transplantation (‘deep anterior lamellar keratoplasty’) should be understood as a general guide to the surgery, rather than an exact description.

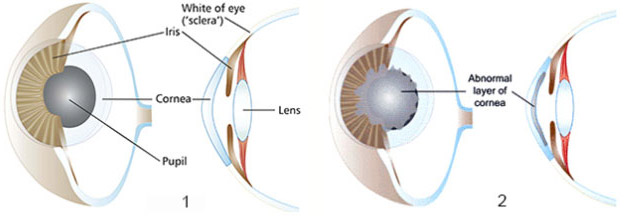
1. In health, the cornea is perfectly clear.
2. The technique is suitable when keratoconus only involves the outer layer of the cornea
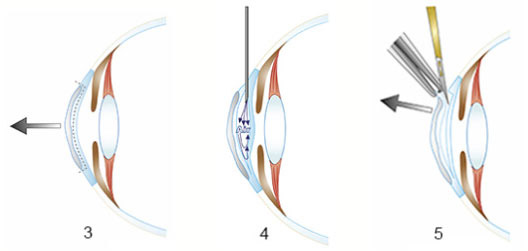
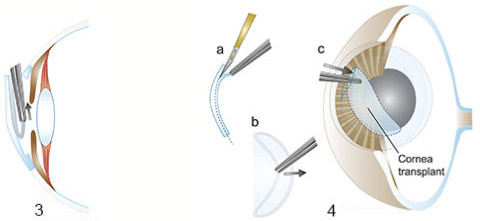
3. The diseased outer layer of the cornea will be removed and replaced.
4. Air is injected into the cornea to seoarate the two layers.
5. The abnormal layer is completely removed
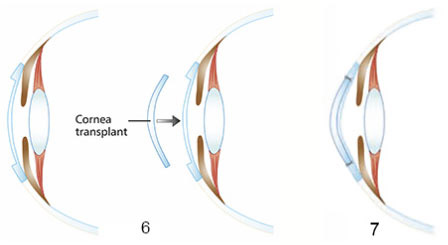
6. A healthy cornea is transplanted into the patient’s cornea to replace the diseased layer.
7. The cornea transplant is secured with ultra-fine sutures
Partial cornea transplantation for Fuchs (‘endothelial keratoplasty’)
Daily Mail on Fuchs
This is a major advance in cornea transplantation for Fuchs as it saves most of the patient’s own cornea. Only the innermost layer (called the ‘endothelium’) is replaced and the outer layer (called the ‘stroma’) is unchanged. This is logical because in Fuchs only the endothelium is diseased and needs replacement – the stroma is perfectly normal and can be left alone. The great advantage of this method is that the donor endothelium self-adheres and is not sutured (stitched) into place. There is no astigmatism, unlike the older technique of full thickness transplantation, so contact lenses are not needed after surgery.
I was the first surgeon to perform the new operation in the United Kingdom.It is also done when the cornea endothelium stops working for other reasons such as herpes virus infection or damage during cataract surgery. The article below, originally written for optometrists, describes it in more detail.
New frontiers in cornea transplantation : selective transplantation of the endothelium via a no-suture, keyhole incision
The cornea is the clear ‘front window’ of the eye. It may be damaged by disease processes such as Fuchs’ corneal endothelial dystrophy or inadvertently during cataract surgery. Damage causes the cornea to become opaque and the eye blind.
The treatment for severe cornea disease is cornea transplantation – the patient’s cloudy cornea is removed and replaced by a clear cornea obtained from a deceased person, a process similar to kidney and heart transplantation. For decades the technique used has been ‘full thickness’ cornea transplantation. This entails the removal of the entire cornea and its replacement by a transplant. Whilst traditional, full thickness cornea transplantation may successfully restore vision, it may also cause complications. These include severe astigmatism (distortion of the focus of the eye, necessitating the wearing of hard contact lenses after the operation), glaucoma (raised pressure inside the eye) and rejection of the transplant (necessitating another operation to replace it). Full thickness cornea transplantation is also undesirable because it requires virtually the entire front of the patients’ eye to be removed and replaced by the transplant – such large scale surgery may be very traumatic to this delicate organ.
Recently, a remarkable new treatment for cornea disease has become available. This is a revolutionary method of cornea transplantation called ‘selective endothelial transplantation’. The ‘endothelium’ is the layer of the cornea which is on the inside of the eye. Many cornea diseases damage only the endothelial layer, the other regions of the cornea remaining clear. Fuchs’ corneal endothelial dystrophy and damage occurring during cataract surgery are examples. Using the new technique only the diseased endothelium is replaced leaving the remainder of the cornea, which is healthy, in place.
Selective corneal endothelial transplantation is performed through a minute incision on the surface of the eye, only about 4 mm wide. This is approximately the same size as the incision made during cataract surgery. The diseased inner layer is removed through this tiny incision. A transplant composed of healthy corneal endothelium is inserted by gently folding it so that it can enter through the incision. Once inside the eye it is carefully manipulated into position and will miraculously adhere to the patient’s own cornea without sutures!
The new technique is greatly superior to traditional, full thickness cornea transplantation. The tiny incision causes much less trauma to the delicate eye. Disabling post-operative astigmatism is eliminated altogether, no sutures are required and recovery after the operation is much faster.
Case study: A 78 year old lady suffers from Fuchs’ corneal endothelial dystrophy. Her right eye received a full thickness cornea transplant several years previously. Sixteen sutures were required to secure the transplant in place. It was 18 months before healing was complete. She can only see from her right eye whilst wearing a hard contact lens which must be inserted every morning and removed before bed.
By contrast her left eye received a selective corneal endothelial transplant a few months ago. Recovery was complete after three months, no sutures were needed and she sees well from her left eye without needing to wear a contact lens.
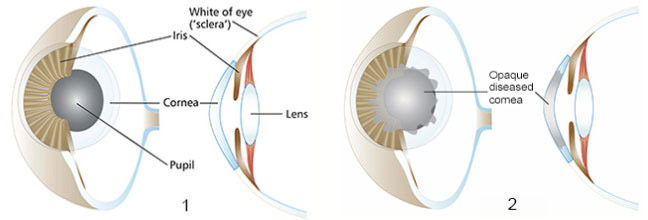
These illustrations of partial cornea transplantation (‘endothelial keratoplasty’) should be understood as a general guide to the surgery, rather than an exact description.
1. In health, the cornea is perfectly clear
2. The technique is suitable when fuchs has famaged the inner cornea layer, the endolithium
3. The diseased endothelium us removed, leaving the rest of the cornea which is normal
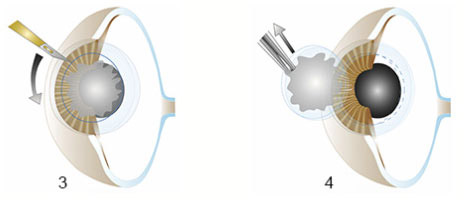
4. A normal cornea will be transplanted into the patient. 4(a) Healthy endothelium is obtained from the donor cornea to match the diseased region the has been removed from the patients cornea. The transplant 4(b) folded and 4(c) inserted into the patients eye via a small incision in the cornea.
5. After insertion, the transplant is unfolded.
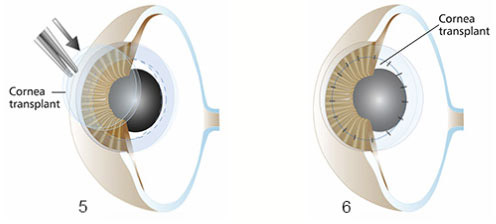
6. Air is injected to position the transplant against the patient’s cornea. Once contact is achived, the transplant will adhere permanently.
7. Post-operative appearance of the cornea transplant (blue region). Sutures are not required to hold the transplant in place.

An opaque cornea prior to selective corneal endothelial transplantation (left). A patient with fuchs after selective endothelial transplantation (right). The cornea is crystal clear.
Full thickness transplantation (‘penetrating keratoplasty’)
The centre of the patient’s own cornea is completely removed and replaced by a transplant which is sutured (stitched) into place.
These illustrations of full thickness transplantation of the cornea (‘penetrating keratoplasty’) should be taken as a general guide to the surgery, rather than an exact description
1. In health, the cornea is perfectly clear.
2. The technique is suitable when keratocunus involves the full thickness of the cornea
3. A circular cut is made into the diseased cornea.
4. The diseased cornea is removed
5. A healthy cornea is transplanted into the space created by removal of the patient’s diseased cornea.
6. The cornea transplant is held place with ultra-fine sutures. These are not visible to the naked eye. The transplant bonds slowly to the patient’s cornea and the sutures are then removed

I performed this full thickness cornea transplant for a patient with advanced keratoconus
Full thickness cornea transplant aftercare: Fairly frequent review in outpatients is required during the first year after the surgery. Eye drops containing steroid and antibiotic are used after the operation for a variable period, generally about 9 months. Unlike other transplants e.g. kidney or heart, tablets to prevent rejection are not needed. However patients with cornea disease caused by herpes virus infection may need long term medication with Zovirax antiviral tablets to prevent recurrence of the virus on the transplant.
The sutures that hold the transplant in place are non-dissolving and need to be removed after 9-12 months. This is not painful and does not need an anaesthetic. It is done in outpatients.
Vision recovery after surgery is usually very slow and can take 9-18 months. It is normally necessary to wear a contact lens to obtain good vision after transplantation. It is not normally possible to see clearly after transplantation with glasses or ‘naked eye’. This is due to astigmatism which is discussed below. The contact lens needs to be a rigid gas permeable (hard) type. Soft lenses do not provide adequate vision.
It is sometimes possible to have refractive surgery after transplantation to reduce dependence on contact lenses. Please see the Eyesite on refractive surgery.
Full thickness cornea transplant potential complications In expert hands the outcome of cornea transplantation is usually good. However it is important to be aware of potential complications which include –
Astigmatism: This is caused by unevenness of the shape of the new cornea after it has healed and is found in virtually every transplant. Astigmatism is not dangerous but does reduce vision. The solution is to wear a rigid gas permeable (hard) contact lens which neutralises astigmatism.
Rejection: The body may reject the new cornea. The chance of this happening depends on features specific to each patient. Rejection causes vision to become cloudy and the eye may be red and sometimes sore. It is usually possible to reverse rejection by prompt administration of steroid eye drops or injections.
Infection: Various bacteria may infect the transplant requiring intensive antibiotic eye drops. Cornea disease caused by herpes virus may reactivate on the transplant causing scarring.
Wearing Out: A cornea transplant can simply wear out because its cells age more quickly than those of a normal cornea. A new transplant is required to replace it.