Helping you see better
During cataract surgery the eye’s natural lens, now cloudy and an impediment to clear vision, is removed and replaced by a lens implant. The cataract is cured . . . but more may be achieved. Sophisticated measurements prior to surgery reveal the unique characteristics of every eye. A customised lens implant chosen to be compatible with your eye neutralises its weaknesses, maximising quality of vision and minimising glasses dependence. Imperfections such as short or long sight, astigmatism and reading glasses may all be treated - provided the optimum lens implant is used. Customised lens implants are the best way to achieve freedom from glasses, especially reading glasses, after surgery.
What is a lens implant?
Lens implants (also called intraocular lenses or ‘IOLs’) are a prosthesis, in this case a transparent plastic lens usually about 6mm in diameter. They are inserted during cataract surgery to replace the focusing power of the natural lens of the eye that has been removed.
The first ever lens implant was made by Rayner in the UK in 1949. It was designed by Sir Harold Ridley FRS FRCS a Consultant Ophthalmologist at St. Thomas’ Hospital London who also performed the surgery. Since then many millions of lens implants have been implanted internationally.
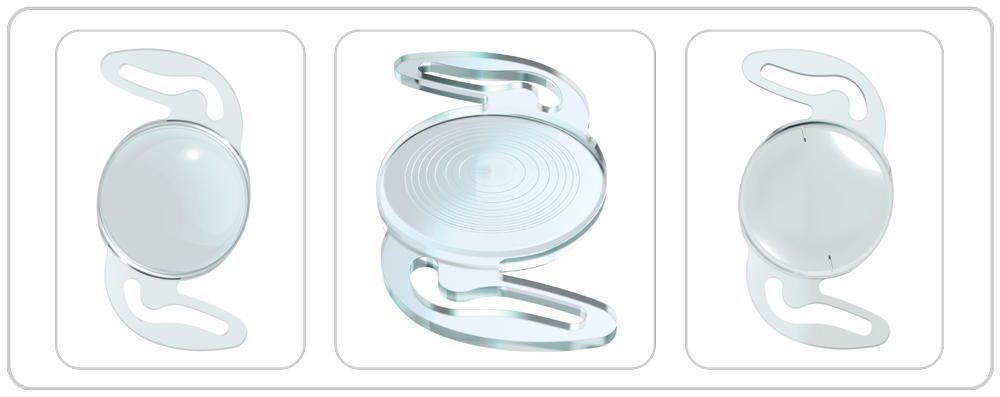
Rayner aspheric monofocal IOL (left). Rayner multifocal IOL (centre). Rayner aspheric toric monofocal IOL (right)
Lens implant technology is amongst the greatest advances made by modern medicine. Before it, clumsy thick glasses, unsightly and affording poor optical performance, were needed after cataract surgery.
Lens implants have improved enormously over the years. Many types are now available to suit different eyes and diverse visual requirements.
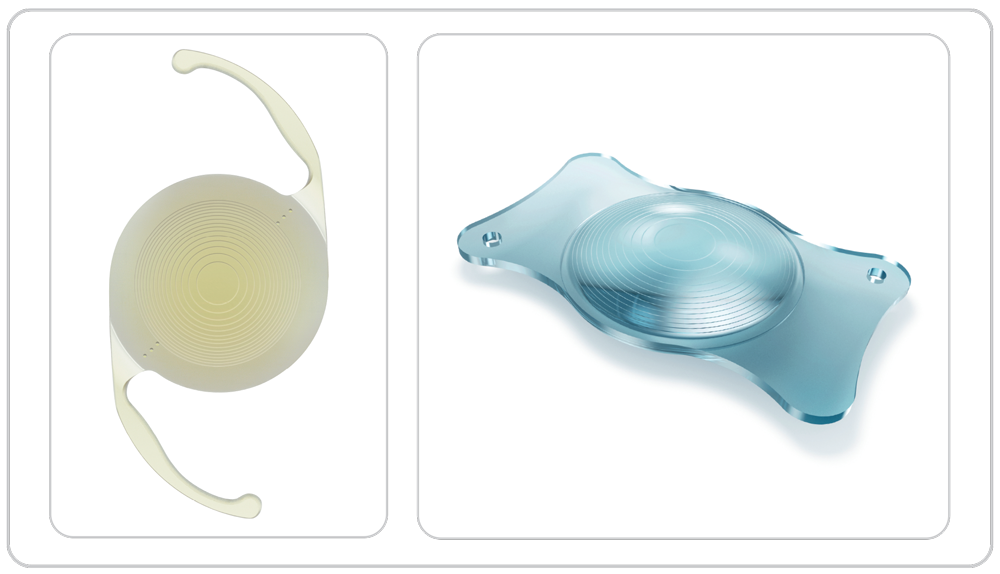
Alcon Panoptix toric multifocal IOL (left). Zeiss extended-depth-of-focus multifocal (right)
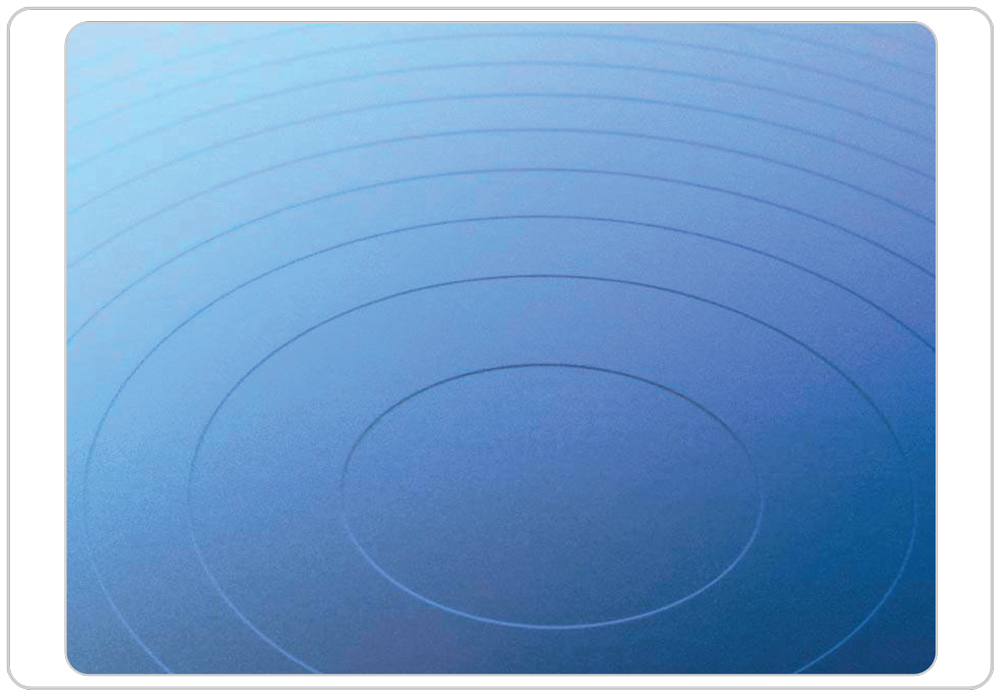
Magnified view of a multifocal IOL showing the complex surface that corrects presbyopia
Choosing the best lens implant for you: the customised cataract surgery approach
I am committed to maximising the quality of your vision and minimising your need for glasses post-operatively. This is achieved in the following way:-
Step 1) Pre-operative measurements
In-depth analysis of your eyes is performed, many of the tests requiring ultra-sophisticated equipment.
Your glasses prescription is determined by an optometrist (optician). Axial length is the front-to-back length of the eye, measured with an optical biometer, a sophisticated laser.

Optical biometer (left). Axial length measurement (right)
The curvature of the cornea is assessed with a keratometer. Extremely fine measurements of astigmatism, the cornea’s higher order aberrations, minute variations in the eye’s direction of gaze and movements of the pupil are made with a topographer.
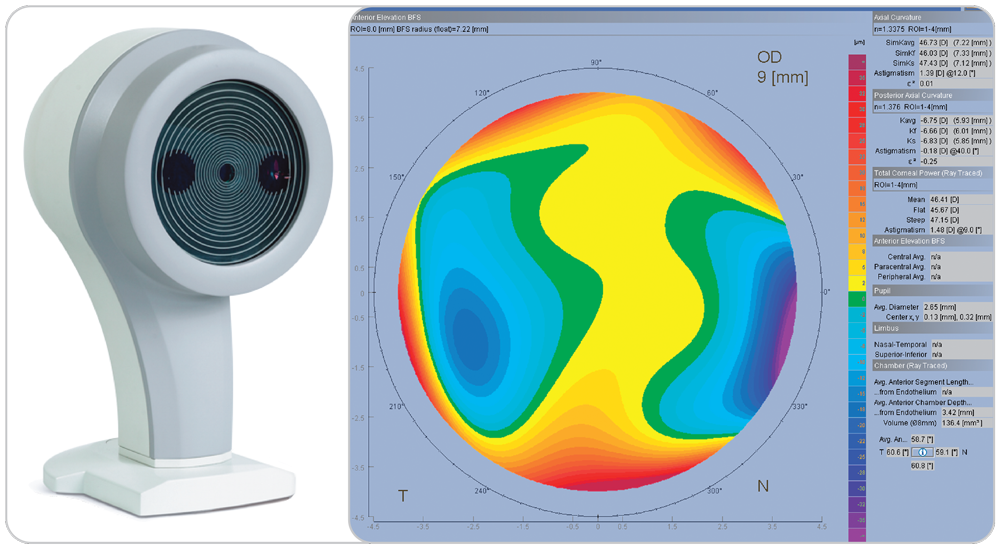
Cornea topographer (left). Cornea topographic map (right)
The health of the cornea and retina, parts of the eye nearby the forthcoming cataract surgery, is respectively determined by a cornea endothelial cell count and ocular computed tomography (OCT).

Endothelial cell analysis of normal cornea
The health of the cornea and retina, parts of the eye nearby the forthcoming cataract surgery, is respectively determined by a cornea endothelial cell count and ocular computed tomography (OCT).
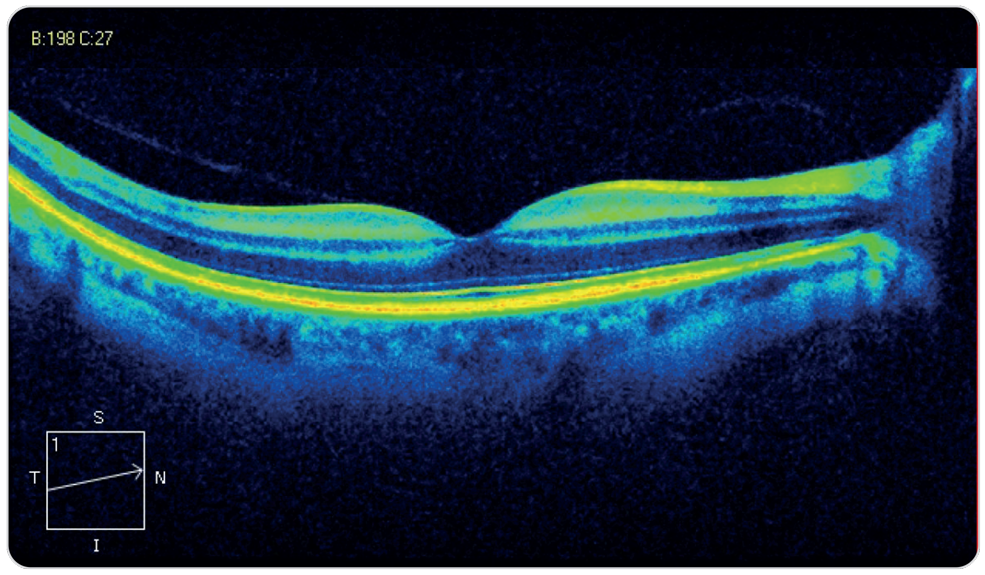
OCT scan of normal retina
Step 2) Pre-operative consultation
After the measurements, I will examine your eyes and ascertain your visual requirements, for example the extent to which you wish to be less dependent on glasses. There will be plenty of time to discuss which lens implant is best for you.
Step 3) Explaining lens implants
Characteristics of the different types of lens implant
For this description, the following approximate definitions apply: ‘far’ means driving, watching TV or cinema, ‘middle’ refers to the car dashboard/sat-nav, desktop computers, eating and cooking and ‘near’ is for reading, make-up and shaving. Seeing your mobile phone may be either middle or near vision depending on how you like to hold it.
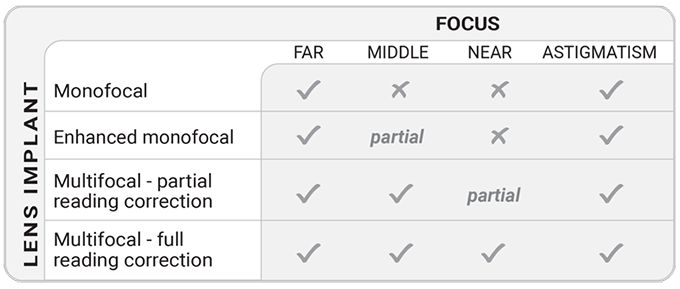
1) Monofocal (also called ‘single vision’) lenses
Focus: either far or middle or near.
Purpose: freedom from glasses at one of either far or middle or near distances. Glasses will be needed for the two distances not focused by the lens.
Comment: Monofocals may sometimes be used with ‘monovision’ in which one eye is focused for far and the other for near. This is a compromise that works in a minority of patients. ‘Toric’ versions of this lens correct astigmatism.
2) Enhanced monofocal lenses
Focus: far + some middle.
Purpose: freedom from glasses at far and less demanding middle distances. With this type of intraocular lens you will need glasses for near and some middle tasks.
Comment: Provide enhanced monovision. Astigmatism-correcting versions of this lens are available.
3) Multifocal with partial reading correction (also called ‘partial multifocal’ and ‘extended depth of focus’) lenses
Focus: far + middle + some near.
Purpose: freedom from glasses at far and middle distances and partial freedom at near, for less demanding tasks. With this type of intraocular lens you will sometimes need glasses for reading, depending on print size and contrast.
Comment: Don’t usually cause problems at night. Are compatible with many eye health disorders. Incorporate astigmatism correction when needed.
4) Multifocal with full reading correction (also called ‘full multifocal’) lenses
Focus: far + intermediate + near.
Purpose: full freedom from glasses at all distances.
Comment: Unlike the other lenses, full multifocals cause glare and haloes at night. This isn’t usually a severe problem and is often temporary but there’s no technology that accurately forecasts which patients will be significantly inconvenienced and there is nothing the surgeon can do to help, short of removing the lens. The quality of vision provided by this lens may be slightly less sharp than other types although the difference is usually too small to be noticeable. Full multifocals are not suitable if you suffer from glaucoma or retina disorders or have had prior laser refractive surgery. Astigmatism correction is provided if needed.
OCT scan of normal retina
Summary of lens implant characteristics
Examples of lens implants customised for my patient’s eyes
- A patient whose priority is complete glasses independence and who doesn’t often drive at night, might receive a full multifocal lens focusing at all distances.
- A patient who requires freedom from glasses at far and middle ranges and who would also value some reading glasses independence, might receive a partial multifocal/extended depth of focus lens. As well as far, these focus the very important middle range (car sat-navs and dashboards, golf, desktop computers, meals). They help too with near vision, but with this type of lens glasses for reading are sometimes needed. This may be the right choice for people who don’t want readers all the time but accept them when settling down to the Sunday newspaper. They may also suit habitual nighttime drivers as they don’t usually cause glare and haloes.
- A patient who doesn’t mind reading glasses but nonetheless considers that a monofocal lens would entail an undesirable dependence on glasses overall, might choose an enhanced monofocal lens providing some useful middle range as well as far focus. This lens may also be used to improve the monovision technique in patients who were successful with it before developing cataract.
Step 4) Surgery
Some lens implants, for example astigmatism-correcting, require highly accurate alignment within the eye if they are to work properly. I use a method of registering the shape of the cornea before the operation begins to achieve this.
Step 5) Post-operative consultation
I will examine you and repeat some of the measurements made prior to surgery, to determine the accuracy of the outcome. I will also ask what you think of your new eyesight!

A non-customised IOL (left) does not correct astigmatism. A customised toric IOL (right)
corrects astigmatism and the patient sees clearly without glasses
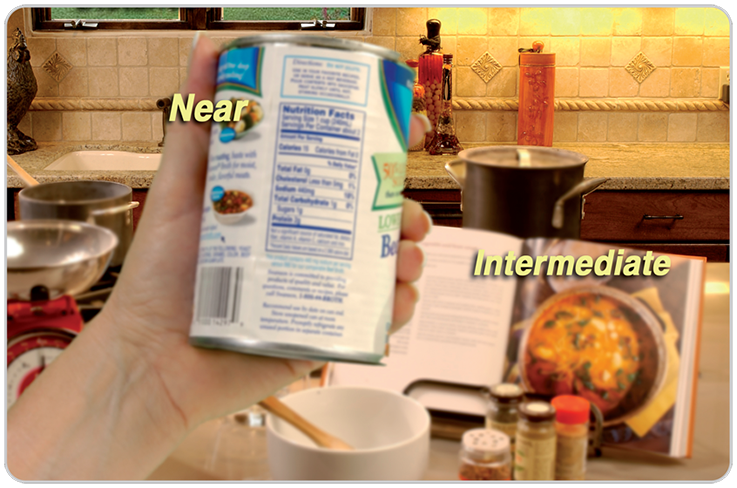
This patient has received a non-customised IOL and cannot read the soup can or recipe
book without glasses

A customised multifocal IOL has been used. Close objects are seen without glasses
(Images above are simulated)